It is not clear whether the order, the president’s third to address the topic in less than a year, has any legal power.
from NYT > Health https://ift.tt/WdyfEmj
from NYT > Health https://ift.tt/WdyfEmj

April Health And Fitness Tips.

Enter April Health And Fitness Tips.

April Health And Fitness Tips.
 RoseRose
RoseRoseLast year, Baltimore had three mass overdose incidents in the span of three months in its Penn North neighborhood.
In one incident, more than two dozen people were hospitalized after many were found unresponsive, lying in the streets or on sidewalks. No one died, but some came close.
Follow-up testing found that the street drugs contained high levels of N-methylclonazepam, a benzodiazepine that operates similarly to Xanax or Valium. Like opioids, benzodiazepines suppress breathing. When they’re combined, the risk of overdose goes up. And benzodiazepines don’t respond to opioid overdose reversal drugs.
Afterward, the Baltimore Harm Reduction Coalition created test strips specifically for benzodiazepines. The group distributed them — along with test strips that identify other harmful adulterants, such as fentanyl, xylazine, and medetomidine — at clinics and neighborhood events. The strips, available at no cost, can also be found in bars and spread out on street corners. People testing drugs mix a small amount with water and then dip a test strip into the liquid. The strip will change color if it identifies an adulterant.
“Nobody really knows what they’re getting whenever they’re getting stuff off of the street,” said Candy Kerr, a spokesperson for the coalition. “Having the test strips available for the general public gives them the option to move slower if they’re going to use whatever they’re going to use.”

But a new federal policy could make it harder for organizations such as Kerr’s to give out the test strips, and they’re worried that overdoses could increase. In late April, the Substance Abuse and Mental Health Services Administration banned the use of federal grants for distributing strips to the public and for some other harm reduction practices that have been credited with saving lives. Test strips have been used for nearly 10 years to identify adulterants.
A letter sent to local health departments and nonprofits that provide addiction services explained that the Trump administration believes those harm reduction practices “facilitate illicit drug use and are incompatible with Federal laws.”
According to the letter, grants from the Department of Health and Human Services also cannot be used for programs that support the use of clean needles or drug paraphernalia such as pipes, or to fund a type of specialized hotline that people can call while taking drugs, so someone is aware and can call for help if they overdose.
The Trump administration wants to focus more on other techniques, such as giving out naloxone, an overdose reversal drug available as a nasal spray, according to Emily Hilliard, an HHS spokesperson.
“It is critical that federal funding provided by the American taxpayer goes to effective, common-sense solutions that have been proven to save lives and keep people out of an endless cycle of addiction and moves them into a life of recovery,” she said.
The new policy does not prohibit federal funds from being used to purchase test strips for use by law enforcement officers, public health officials, EMTs, or other medical professionals.
That creates an important exception for government agencies that test drugs and send out regular reports on what adulterants are saturating the drug supply in certain locations.
Still, Yngvild Olsen, who oversaw SAMHSA’s Center for Substance Abuse Treatment in the Biden and Trump administrations, says there is a substantial body of evidence that shows giving test strips to people who use drugs can change behavior.
“There’s some people deciding not to use the substances, some people deciding to reduce, to use less, or take other types of precautions, including naloxone, and making sure that there are people around that can actually then help in the case of an overdose,” Olsen said.
Kerr said the best approach would be to continue to promote the use of test strips while also continuing to give out lifesaving medications like naloxone. She believes that working on all fronts has helped lead to Baltimore’s decline in overdose deaths, which have dropped more than 40% since 2023.

Under the new policy, nonprofits will still be able to hand out test strips, but they will have to find other funding for that work, which Kerr finds worrisome.
“We’ve been making these strides forward because we’ve had these things, because we’ve been funded,” she said. “We’re going to have to pull money from other places.”
To pay for the test strips, Kerr said, the Baltimore Harm Reduction Coalition will have to cut back on services such as giving out hygiene and wound care kits. But she said that option is better than risking another mass overdose in Baltimore — or allowing even just one preventable fatality.
This article is from a partnership that includes WYPR, NPR, and KFF Health News.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.This article first appeared on KFF Health News and is republished here under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
RoseRoseDoula Taja Iglesias and her business partner have built a space in Alexandria, Virginia, that’s all things pregnancy, birth, and childcare.
Comfortable couches in one area invite expectant parents to settle in for birth education classes. In another, a colorful pile of toys await the babies and toddlers. And there’s a free supply of diapers and food. Years ago, as Iglesias was giving birth and expressing her wish not to have an epidural for pain, she felt isolated and that her preferences were dismissed by the medical staff. Today, she works hard to make sure other parents can have the support of a doula.
“We kind of created this to fill the gaps that we realized existed because we had to go through it,” Iglesias said. She’s the founder of The Momager Co., a doula agency dedicated to giving parents care throughout the perinatal process.
Iglesias said one of the widest gaps is the lack of access to doula care for parents on Medicaid.
Doula care has been associated with improved breastfeeding initiation and less maternal anxiety. The perinatal doula care covers education about pregnancy and birth, advocacy for new parents in the hospital, and help after delivery with lactation and recovery. Doulas often work alongside doctors or midwives who provide medical care.
“The doula is the person that already knows what you want. We know what your dream birth is,” Iglesias explained. “We’re somebody that is standing on the side of the parent.”


Can’t see the audio player? Visit kffhealthnews.org to listen.
In 2022, Virginia became the fourth state to start reimbursing doulas through Medicaid. A push to address the country’s maternal mortality rates, which are higher than in other high-income countries, has been an engine for lawmakers looking to give women on Medicaid the support of doula care. For example, another Virginia law requires hospitals to allow an extra person, other than a family member, in the delivery room.
The services offered and the number of visits covered by Medicaid vary by state, but today doulas are covered in 26 states and Washington, D.C. An additional 20 states have considered proposals or are in the process of implementing similar policies.
In Virginia, doulas say the administrative and logistical challenges they encounter are trickling down to moms. A review of the Virginia Certification Board’s Doula Registry this June found just 19 doulas based in Northern Virginia accept payment from Medicaid.
Doulas say that while Medicaid coverage of their services is a good first step, the amount of paperwork required in the approval process and the low reimbursement rates mean that fewer doulas participate in the Medicaid program, reducing access for beneficiaries.
A 2021 law that extended doula benefits to Medicaid enrollees sought to improve the health of Virginia parents and decrease the number of mothers who die during the time surrounding birth. The state’s maternal mortality rate is among the nation’s highest.
As co-chair of the state’s task force on doula regulations, Iglesias helps shape policies that make it easier for moms on Medicaid to get doula care through the program.
To access doula services in Virginia, parents on Medicaid must have a referral from a doctor, and their doula must be approved by the state to care for Medicaid beneficiaries. Iglesias would like to see that process be quicker and less costly for doulas, who pay $75-$150 for certification.
While the policy debates continue, Iglesias has decided not to get certified to care for parents on Medicaid. Instead, she raises money to provide doula care for parents on Medicaid outside the system.
“I don’t want to be state-certified with a training that I feel is not full and complete, a training that doesn’t touch on that community aspect of work,” she said.
Iglesias said the services covered are too limited and Medicaid does not allow her to work with clients as she sees fit. Virginia’s payment covers up to eight doula visits. All but the first visit are limited to one hour, which Iglesias said isn’t enough time.
“If you want to actually build a relationship with this person that you’re going to be standing in with in their most vulnerable moment, it ain’t happening,” Iglesias said.



While pursuing her PhD at George Mason University, Desirae Leaphart Mensah studied the initial implementation of the doula reimbursement policy in Virginia.
Mensah collected data from 2022 to 2024 for a study published this year. She interviewed doulas eager to serve clients on Medicaid. But some told her they got bogged down in the paperwork and never were certified. Doulas report similar struggles with the certification process today.
Mensah said the mismatch between the size of the Medicaid population in Northern Virginia and the low number of doulas available leads to fewer parents receiving doula care.
Coverage is a good first step, Mensah noted, but it doesn’t translate to enough access. During the first two years of implementation, fewer than 1% of Medicaid births in Virginia used doula services. That study is the latest available.
Kenda Denia, executive director of Birth in Color, a statewide doula collective in Virginia, welcomed the law at first.
“But now we’re looking at certain logistics that are not working,” Denia said.
Private-pay doulas in Virginia commonly charge $1,200 to $3,000 per pregnancy. For families wanting more extensive prenatal or postpartum services, the fee can be as much as $6,000. Virginia’s Medicaid program, also known as Cardinal Care, reimburses doulas $859 per pregnancy. They receive an additional $100 if their client attends prenatal and postpartum doctors’ visits.
The pay is too low and does not reflect the value of the services they provide, Denia said. “Midwives don’t get paid this. Doctors don’t get paid this,” she explained. “We are driving to people’s homes for postpartum and prenatal care.”
Doulas might wait weeks or months for reimbursement, and the pay is not flexible. The Medicaid reimbursement rate is the same across the state and does not capture the higher cost of living in areas like Alexandria. It’s roughly 32% more expensive in Alexandria than the average cost of living in Virginia, according to ERI Economic Research Institute, a private data analytics group.
Despite the barriers, Denia applauded parts of the policy. Medicaid coverage of doulas means that more parents can have a “birthing bestie,” she said.
Before getting pregnant, Juliana Navia had no idea what doulas did. But while at a free clinic for her prenatal checkups, Navia connected with Iglesias. Later, Iglesias became Navia’s doula and helped her navigate a difficult situation when she wasn’t getting the kind of care she wanted at the hospital.
“I was stressed giving birth, but my doula helped me,” Navia said. “I was advocated for.”
This article first appeared on KFF Health News and is republished here under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
RoseRoseRose
Céline Gounder, KFF Health News’ editor-at-large for public health, discussed the cyclosporiasis outbreak on CBS News’ CBS Mornings on Aug. 5. Gounder discussed New Mexico’s measles outbreak on CBS News 24/7’s The Daily Report on Aug. 4. She also discussed peptides on Ideastream Public Media/WKSU’s Sound of Ideas on Aug. 3.
KFF Health News chief Washington correspondent Julie Rovner discussed the end of a Biden-era Medicare Part D subsidy on WBUR’s Here & Now on Aug. 3.
KFF Health News Southern correspondent Sam Whitehead discussed the new medical frailty work requirements on WUGA’s The Georgia Health Report on July 31.
This article first appeared on KFF Health News and is republished here under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
RoseRoseSay you live in deep-red Louisiana, a state that has effectively banned abortion. It may be easier for you to get abortion pills now than before the Supreme Court overturned Roe v. Wade. Here’s why — and what it means for future battles over abortion access.
And as a federal court mulls a case that could result in significant restrictions on a pill used in most abortions, healthcare providers say they have alternatives to preserve access even in states with bans in place. Read more here.
This article first appeared on KFF Health News and is republished here under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
RoseRoseRoseRoseRoseRoseRoseAMHERST, Mass. — For the last 30 years, whenever pediatrician John Snyder wanted to find the most up-to-date research on treating young patients, he would turn to the Centers for Disease Control and Prevention.
If he wanted to learn more about an outbreak of measles or hantavirus, he would pore over the weekly CDC report that came by email. If a patient’s family was traveling to Africa or Asia, he would check the latest CDC vaccine recommendations for overseas travel. And if a family was worried about potential side effects from a shot, he could always send them to the CDC’s website to bolster his argument to get the immunization.
Public trust in the CDC has hit bumps in the road during infectious disease outbreaks, but for medical professionals, Snyder said, “the CDC used to be, worldwide, the most trusted source of information pertaining to public health and infectious disease.”
Yet even doctors began losing trust, Snyder said, after Donald Trump was elected president again. Trump quickly tapped longtime anti-vaccine activist Robert F. Kennedy Jr. as his nominee to lead the Department of Health and Human Services, which oversees the CDC.
Within months of his confirmation as secretary, Kennedy had dismissed every member of the CDC’s vaccine advisory board and replaced them with new appointees, some of them prominent vaccine skeptics.
“It turned into a completely unreputable source of information,” Snyder said.
This rupture of scientific trust in the CDC has put many pediatricians like Snyder in a bind, as they no longer turn to the country’s preeminent public health agency and instead search for ways to fill the information gap. Some doctors are launching their own vaccine education efforts, sometimes in collaboration with local public health departments.
On Jan. 5, the CDC removed some vaccines from the recommended vaccine schedule for all children — against the advice of major medical groups like the American Academy of Pediatrics. The number of recommended vaccines shrank as the agency dropped rotavirus, covid-19, influenza, hepatitis A, hepatitis B, and meningococcal disease from the list. The agency did not respond to a request for comment for this article.
In March, after medical groups sued, a federal judge ordered the Trump administration to revert to the previous guidelines. The administration has appealed the judge’s decision.
The back-and-forth “creates a whole bunch of confusion in the public,” Snyder said. “And it’s very confusing even for healthcare providers.”
So he’s trying to be clear to patients about what the evidence shows, even if that means going against the federal government. His practice, Amherst Pediatrics, changed its website to say: “The CDC is no longer considered to be a reliable or legitimate source of information.”
“It’s shocking that we have to say that,” Snyder said. Instead, the site directs families to get information from their own doctor, the state of Massachusetts, or nongovernmental medical organizations including the AAP.
In the exam room, Snyder is having more tense conversations with families. He said some parents are explicit that they want to hew to what the CDC recommends. “Even if they don’t say that, we have definitely seen increasing hesitancy and questions,” he said. “All of that interferes with us protecting children.”
On a spring afternoon, several of Snyder’s young patients came into Amherst Pediatrics for routine visits.
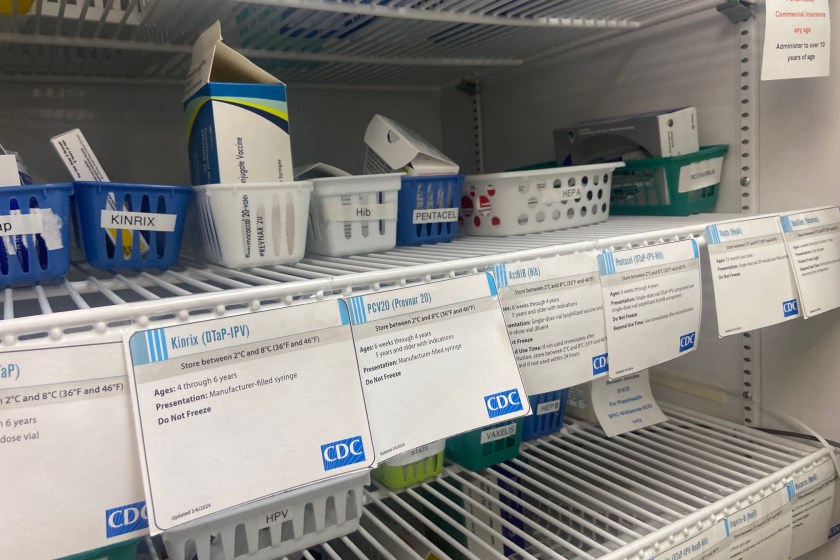
“Let’s talk about vaccines,” Snyder said to one mother, Tenzin Dekey, who was there with her 1-year-old. Snyder explained that her son was due for the MMR vaccine, which protects against measles, mumps, and rubella, in addition to the chickenpox, hepatitis A, and flu vaccines.
“So that’s four shots, two in each leg,” he said, as he handed Dekey CDC information sheets about the vaccines. She glanced at them and agreed to the shots.
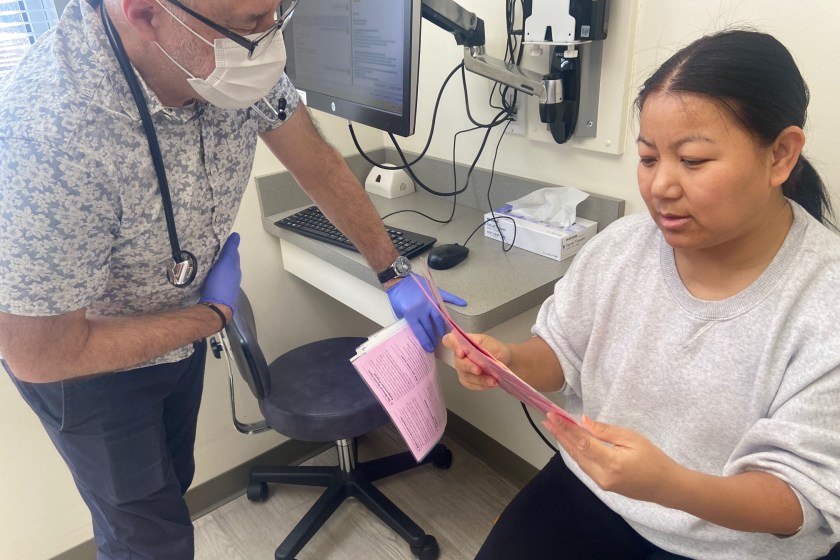
Ironically, the information sheets are stamped with the CDC’s logo — as required by law — even though Amherst Pediatrics has explicitly directed patients away from the CDC. Snyder said he hates that disconnect.
“This has been a source of heated discussion,” he said. “How can we be saying, ‘Do not trust the CDC when it comes to vaccines,’ yet here is the information we’re giving our own patients when they’re in the office about vaccines?”
Another mother brought her 14-year-old son for his annual physical. She asked to be identified by only her first name, Melissa, so she could freely discuss her family’s private health issues.
Snyder recommended the HPV vaccine, which helps prevent some cancers. Although Melissa had refused the HPV vaccine in a previous visit, this time she left the decision up to her son. He agreed to it. But for other vaccines, she wouldn’t budge.
“I’m a hard ‘no’ on the covid,” she told Snyder.
“We could talk about that if you want,” he suggested.
“I don’t need to talk about it,” she replied.
After the appointment, Melissa said she just doesn’t know whom to trust anymore when it comes to vaccine safety. She used to get information from the CDC but no longer does.
“I worry that it’s been politicized a lot, and I don’t like politics,” she said. “Now I prefer to hear things from people, healthcare professionals.”
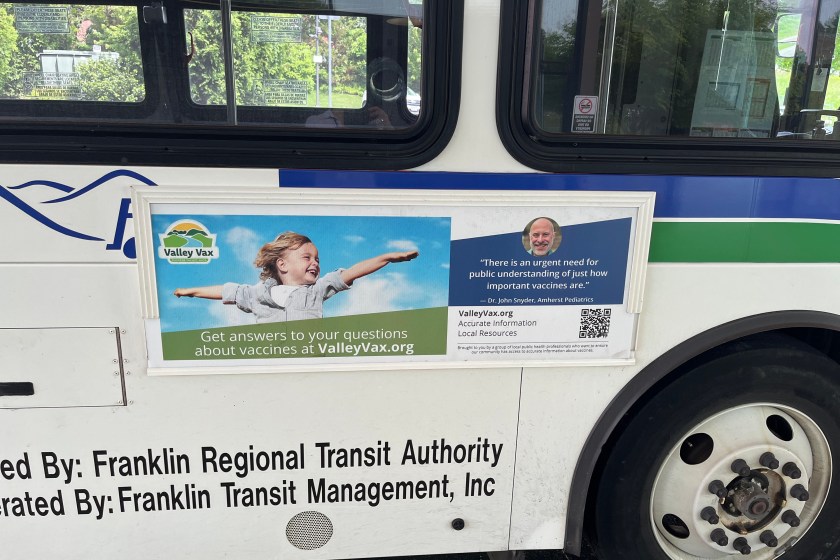
Such distrust and confusion inspired Snyder to join an independent vaccine information campaign, along with other pediatric practices and health departments in the Connecticut River Valley of Western Massachusetts.
The campaign’s website, which is promoted in Snyder’s waiting room, is called Valley Vax. It sidesteps the CDC and highlights advice from local doctors and national medical groups, including the AAP. Valley Vax bought ads on the sides of buses in Western Massachusetts to promote the site, with the faces and testimonials of local doctors including Snyder.
“We wanted something that felt familiar and appealing and that they might be more likely to trust,” said Kiko Malin, director of Amherst’s public health department, who coordinates the Valley Vax effort.
She said the organizers decided not to criticize the CDC outright.
“Some information from the CDC is reasonable. Like they are doing a good job of tracking influenza-like illness rates in the country,” Malin said. “It’s important not to discount an organization completely.”
Still, she said it’s the first time she’s had to contradict health information from the CDC. “That’s not a comfortable place to be in at all,” she said.
Other health leaders are also banding together to get out evidence-based information. At the state level, California, Hawai‘i, Oregon, and Washington — frustrated with the CDC — operate the West Coast Health Alliance to “ensure the public has access to credible information.” And governors of 14 states and Guam set up the Governors Public Health Alliance in response to declining trust in federal health agencies.
Locally, some public health departments are partnering with community leaders to reach people who have stopped listening to government institutions but “do have strong connections within their faith community or do have strong connections within their neighborhood,” said Adriane Casalotti, a spokesperson for the National Association of County and City Health Officials.
Like Amherst, many local health departments now direct people to professional medical organizations instead of the CDC, Casalotti said, because advice from those groups may change slightly as the science evolves, but it’s unlikely to change with each lawsuit against the government.
This article is from a partnership that includes New England Public Media, NPR, and KFF Health News.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.This article first appeared on KFF Health News and is republished here under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
RoseRoseMore than 900 people in Washtenaw County, Michigan, have been sickened with cyclosporiasis since mid-June. Linda Kim, a public health nurse, has called more than 100 of them. Almost everyone has said the same thing: It’s excruciating, and one of the worst illnesses they’ve experienced.
But on a Wednesday in July, she called one man who said he wouldn’t mind having it again, actually.
“You’re enjoying the weight loss?” Kim said, laughing as she took notes in a small conference room at the Washtenaw County Health Department building, just outside Ann Arbor. “Well, I’m glad to hear that. At least you got something good out of it!”
Normally, Kim’s supposed to be working downstairs in the clinic, where families wait in gray plastic chairs in the lobby for free or low-cost immunizations. But she hasn’t been there in months.
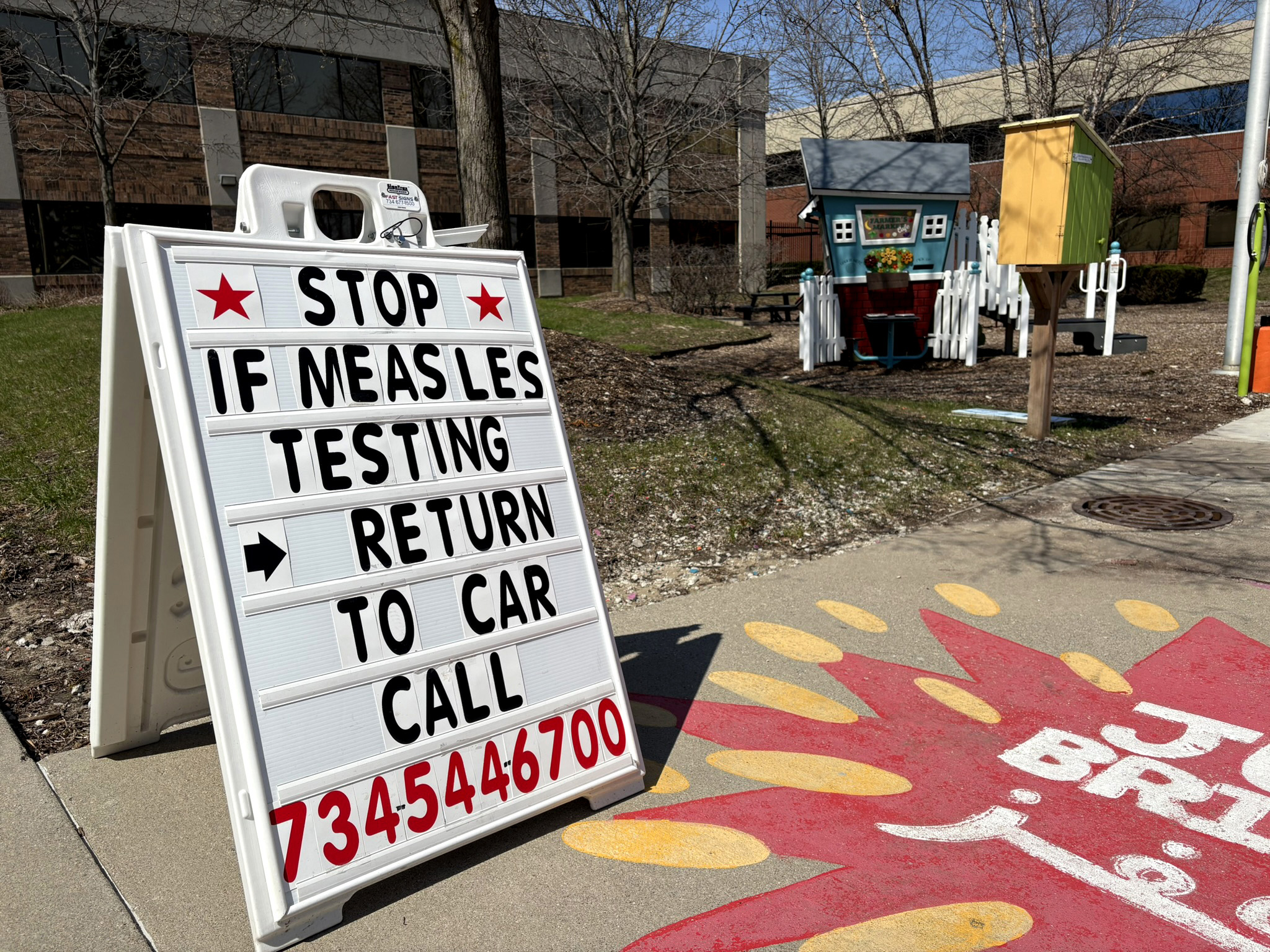
In March, Kim was transferred to a different department to help deal with a measles outbreak that sickened seven people in the county, five of them children. It was an all-hands-on-deck situation; everyone worked overtime. The state issued an advisory urging families in Washtenaw and surrounding counties to get babies 6 months or older vaccinated ahead of schedule, if possible.
The contact-tracing calls for measles could be contentious, Kim said. People were suspicious, asking her how she knew they had tested positive, or why they should give her any information.
“People were like, ‘Oh, you’re just trying to restrict my life,’ or ‘You’re just trying to get information out of me and get me in trouble,’” she said. “It’s like, no, we’re actually not doing that at all.”
As she tried to explain to them, tracing the spread of the highly contagious virus and publicizing possible exposure sites was an effort to “keep it contained, so it doesn’t become something huge.”
The county’s measles outbreak ended in late May. Then in June, reports of cyclosporiasis cases started pouring in — more than 11,000 so far in Michigan, including two deaths. Both people who died had “significant underlying health conditions that may have been impacted by cyclosporiasis and dehydration,” the state health department said on its website Aug. 3. Health officials aren’t providing more details, department spokesperson Lynn Sutfin said in an email, but are stressing that cyclosporiasis generally isn’t life-threatening and that deaths from it are uncommon in the U.S.
Kim said the cyclosporiasis surveillance has been very different from her experience with the measles outbreak. Now, people seem eager to divulge even the most graphic details, such as “pooping their beds, and, like, putting down towels and it’s not enough.”
Since she’s a nurse, such confessions don’t faze her, she said. Still, staffers have hundreds of these calls to make, so they try to keep each conversation under an hour.
But foodborne illness investigations are complex. Especially for this parasite, cyclospora. Symptoms can take as long as two weeks to appear after people have eaten contaminated food. And no one remembers what they ate two weeks ago, public health staffers said.
The interview process can be extremely detailed. Kim and her colleagues ask people to pull up their restaurant receipts, scroll through purchases on their grocery store apps, even try to recall details such as the exact brand of bagged salad mix they bought, or the type of taco they got at Taco Bell.
“Is that the crunchy one or the soft one?” Kim asked on a recent call, typing on a laptop decorated with cat and vaccine-themed stickers.
Kim has been working with the health department for two years, a period defined by federal funding cuts.
Laina Stebbins, a spokesperson for the Michigan Department of Health and Human Services, said the Trump administration’s sweeping cuts to public health grants eliminated a contract between the state health department and 44 of the state’s 45 local departments that funded 123 full-time employees.
Those cuts also affected the state’s disease surveillance labs, “reducing funding for equipment maintenance contracts, data modernization, and the ability to innovate laboratory processes during emerging disease response,” Stebbins said.
Some of that funding was restored after Michigan won a temporary restraining order against the Trump administration. But Washtenaw’s health department still had to scale back some disease surveillance and outbreak response work. Currently, employees who leave or retire aren’t replaced, except for those on the nursing team, which is hiring but still understaffed.
The county’s Health Equity Council, which aims to reduce health disparities, including in mental health, was shuttered suddenly in early 2025. Nearly a year later, it resumed its work, with funding at least through this September.

An employee from the Centers for Disease Control and Prevention had been stationed at the department. During the funding chaos, the worker was fired, then rehired, then furloughed.
The federal response to cyclosporiasis has felt frustratingly slow, according to Christina Zilke, a nursing supervisor at the Washtenaw health department.
“It took them forever to say that this was lettuce, and fast-food restaurants were taking it off the shelves before the CDC ever said what it was,” she said.
During a July 14 press call, the deputy director of the CDC’s Division of Foodborne, Waterborne, and Environmental Diseases, Gwen Biggerstaff, said it’s not unusual for it to take a long time to identify a specific source for cyclosporiasis — if it’s identified at all. That’s partly due to the lag time between exposure and the appearance of symptoms, and the complexity of tracing this particular parasite.
Meanwhile, Zilke’s been stocking the coffee station and bringing in pizza, trying to keep up staff morale. It’s not a reward, she said. “It’s more like: ‘Here’s some food for survival. Here’s a break so you don’t quit.’”
Kim, for her part, remains enthusiastic about the job but said it’s been a surreal introduction to a public health career — first measles, now cyclospora.
“If nationally they don’t know what’s going on, how are we locally expected to know what’s going on?” she said. “And also just frustrating to be, like, ‘Wow, I don’t think even our government knows how important public health is.’”
But there’s no time to dwell. She has to move on to the next call, as soon as she can wrap up this one. She gives each person her work number, so people can call or text with any follow-up questions.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.This article first appeared on KFF Health News and is republished here under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
RoseRoseAmanda DeSimone-Shabrack relies on a home healthcare aide to help her high-needs autistic 12-year-old son. Virginia’s Medicaid program covers the assistance, enabling her to work as both an education technology specialist and a professor, run errands, and keep Mason in the home.
That could change. In June, the Department of Justice issued a legal opinion saying federal disability rights laws don’t require states to provide services that allow people with disabilities to remain in their homes rather than institutions.
It’s a sharp reversal from 1999, when a landmark Supreme Court ruling held that unjustified institutionalization constituted discrimination under the Americans with Disabilities Act. Previous administrations have relied on that ruling to enforce civil rights for disabled people, but the Trump administration says that long-held interpretation is wrong.
Advocacy groups say legal protections for about 40 million adults and 5 million children who have disabilities could be undermined, and they worry that the new interpretation may herald a return to forced institutionalization.
The stage is also now set for a legal fight between advocates, states, and the federal government. Some states with ongoing lawsuits challenging disability rights requirements are already citing the DOJ opinion in hopes it will help them prevail.
In a case in Texas, for example, some Republican-led states are arguing that a rule instituting a 1973 civil rights law that led to community and home integration of people with disabilities is costly and infringes on states’ rights.
People like DeSimone-Shabrack are especially worried because, they say, the opinion follows a spate of White House and Republican-led initiatives that have already begun eroding hard-won protections for people with disabilities.
“I’m worried. Am I going to have to put him in an institution, and what’s that going to be like for him?” said DeSimone-Shabrack, whose personal home care help was recently reduced from 30 to 18 hours a week by the state. “As he gets older, am I going to be able to care for him without this support?”
The Department of Health and Human Services remains steadfast in enforcing federal civil rights laws, agency spokesperson Emily Hilliard said in an email.
“Our commitment to ensuring that individuals with disabilities are treated with dignity, afforded equal opportunity, and are able to meaningfully access community services remains unchanged,” she said.
But advocacy groups say the DOJ opinion could have sweeping repercussions. The opinion doesn’t change existing law, but advocates worry that HHS and the DOJ could begin rescinding guidance and regulations that mandate integration for people with disabilities.
They’re concerned that agencies will stop enforcing disability laws that ensure people aren’t unnecessarily institutionalized. HHS, for example, has historically investigated disability discrimination claims at hospitals and in states that get federal funding, enforcing compliance with home and community integration through voluntary agreements. Disability rights experts say those agreements could now be imperiled.
And some states facing financial pressures may roll back Medicaid services that enable people with disabilities to stay in their homes and communities — a trend that’s already happening following last year’s passage of the One Big Beautiful Bill Act, which cuts a projected $900 billion-plus from the safety net program over a decade.
Democrats are seizing on the opinion, which was released in a DOJ memo, to portray President Donald Trump and Republicans as a threat to people with disabilities. Sen. Tammy Duckworth (D-Ill.) and other Senate Democrats led the introduction of a resolution calling on the DOJ to rescind the opinion.
“The Trump Administration’s memo is an outrageous attack on the rights and independence of the disability community,” Duckworth said in a statement.
The DOJ didn’t return emails seeking comment.
According to the DOJ’s interpretation, regulations that give disabled people the right to demand certain services for daily living — bathing, mental health counseling, and financial budgeting help, for instance — and that require states to extend community-based services to mentally disabled individuals are unlawful, a view the agency acknowledged “is out of step with the common understanding of that decision within the federal courts.”
States may have legitimate reason to treat mentally disabled people in institutions, “including resource constraints, capacity limitations in community-based facilities, and safety concerns for both the patient and the community,” the memo reads.
The Supreme Court case, Olmstead v. L.C., has long shaped federal policy. And while it remains to be seen how courts will respond to the DOJ, some states seeking to curtail disability protections see the opinion as significant.
Consider the 2024 lawsuit in federal court in the Northern District of Texas by Republican-led states arguing that an HHS rule about the integration mandate is unlawful. The lawsuit began with broader claims and 17 state plaintiffs. Following significant advocacy from the disability community, only Texas, Alaska, and Florida remain.
Following the new DOJ interpretation, the states filed documentation to inform the court about the memo as a new and relevant development. Similar documentation citing the memo has been filed in disability rights cases in Florida and New Hampshire, according to The Arc of the United States, a disability advocacy group.
Advocates for people with disabilities say the speed at which plaintiffs are citing the opinion underscores how it may be used to justify the erosion of protections.
“The administration’s attempt to dismantle decades of progress in community integration is alarming and inconsistent with federal disability rights laws and Supreme Court precedent as well as the critical enforcement work of prior administrations,” said Shira Wakschlag, senior executive officer of legal advocacy and general counsel at The Arc.
Forced institutionalization led to human rights violations, segregation, and a eugenics movement in the late 19th and early 20th centuries that included involuntary sterilization.
Exposure of the abuses, legal battles, and an independent living movement caused a major shift toward integration. Fewer than 1% of people with intellectual or developmental disabilities lived in state-run facilities in 2021, down from almost 30% in 1967, according to data from the University of Minnesota’s Residential Information Systems Project, which maintains metrics on such long-term services and supports.
The Trump administration has already taken steps to reverse that trend, advocates say.
Trump signed an executive order last year that addresses homelessness by expanding involuntary treatment and institutionalization, reversing a “housing first” approach championed by the Biden administration.
Much of the special education program office is moving from the Department of Education to HHS, raising concerns among advocates that the administration is reverting to a view that disabilities are a medical issue to be fixed rather than differences that can be accommodated.
And cuts in federal funding for Medicaid, a federal-state insurance program for people with low incomes or disabilities, also portend fewer resources and services. States have responded by reducing some optional benefits such as home health aides and support. In addition, qualifying for an exemption from the program’s work requirements, which take effect Jan. 1 in most states, will pose significant hurdles for people with disabilities.
The June DOJ opinion, advocates say, could accelerate the shift and result in court rulings that chip away at disability rights.
“While it doesn’t overnight change the law, it’s very troubling and very dangerous,” said Zoe Brennan-Krohn, director of the Disability Rights Program at the American Civil Liberties Union. “It reflects a really deeply held disrespect for disabled people from this administration and a total lack of awareness of the lived experiences of people with disabilities who are living in their homes.”
Data shows there can be benefits to involuntary institutionalization. Relative to those voluntarily admitted, people with psychiatric illness who were involuntarily admitted “experienced greater improvements in symptoms and function,” according to a September 2024 review in Psychiatry, Psychology and Law, a peer-reviewed academic journal.
Deinstitutionalization has created new challenges. More hospitals have been forced to board people with psychiatric illness in emergency rooms because of a dearth of available beds. And moving people into home- and community-based living was supposed to be accompanied by an increase in outpatient care and treatment that never materialized, creating gaps in support.
But advocates for the disabled community say involuntary institutionalization strips people of their autonomy and poses a higher risk of neglect and abuse.
Jennifer Kucera, 57, of Cleveland, spent two years in a nursing home. She has spinal muscular atrophy, a genetic disease that kills motor neurons, leaving her able to move only part of her left arm and her head.
At the institution, she said, she felt bored and trapped and developed intense itching from scabies, which is caused by microscopic mites.
For more than a decade, however, she has lived in an apartment with the help of caregivers who come in the morning to get her dressed and ready and return to put her to bed. She works at a disability rights group, and her care is covered by Medicaid.
“The two years I lived in the nursing home, it was the most horrible time in my life,” said Kucera, who worries about the DOJ opinion on Olmstead. “My future is a shaking floor beneath me. With the stroke of a pen, they could get rid of everything I’ve built for myself.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.This article first appeared on KFF Health News and is republished here under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
RoseRoseRoseCéline Gounder, KFF Health News’ editor-at-large for public health, discussed how children’s caffeine consumption is affecting their health on CBS News’ CBS Mornings on July 30.
KFF Health News senior correspondent Arthur Allen discussed the recent Anthony Fauci Senate hearing on CBS News 24/7 on July 29.
KFF Health News chief Washington correspondent Julie Rovner discussed the Fauci hearing on WBUR’s Here & Now on July 29. Rovner also discussed exceptional Affordable Care Act enrollment in New Mexico on KJZZ’s The Show on July 29.
KFF Health News national public health correspondent Amy Maxmen discussed the FDA potentially easing restrictions on peptide drugs on CBS News 24/7 on July 24.
KFF Health News Georgia correspondent Briah Lumpkins discussed the local impact of the loss of Environmental Protection Agency grant money on WUGA’s The Georgia Health Report on July 24.
KFF Health News Hawaiʻi correspondent Ashley Mizuo discussed the challenge of finding placement for prisoners after their compassionate release from detention on Hawaiʻi Public Radio’s The Conversation on July 22.
This article first appeared on KFF Health News and is republished here under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
RoseA handful of former public health officials are campaigning for top statewide offices across the country, testing whether their experience with covid and other hot-button health issues will appeal to voters in November.
The officials, all Democrats, are running at a time when the Trump administration is reducing government funding for scientific research, restricting access to some vaccines, and making it more difficult for some Americans to obtain health insurance.
Shaughnessy Naughton, president of 3.14 Action, a political action committee that recruits Democratic candidates with science and health backgrounds, said it is unusual to see so many public health leaders running for office.
“But it’s not surprising given the moment we are living in, with an arsonist running HHS working to undermine the vaccine schedule and public health at large,” she said.
Health and Human Services Secretary Robert F. Kennedy Jr. is a longtime anti-vaccine activist who disparaged public health measures implemented during the pandemic, going as far as calling the covid vaccine the “deadliest vaccine ever made.”
Neither HHS nor the White House responded to requests for comment.
Several of the candidates benefit from name recognition built during the covid pandemic, political science scholars say, when daily news briefings from local health officials became must-see-TV for many citizens sheltering in place from the novel virus. But that cuts two ways.
While many Americans regarded public health officials as offering prudent advice and a steady voice, others criticized them for pushing school closures, mask mandates, and new, quickly created vaccines. The attacks have escalated under President Donald Trump, with Republicans targeting pandemic-era public health leaders such as Anthony Fauci with investigations and a former Fauci adviser even facing criminal prosecution.
National polls show healthcare is top of mind for many voters this year, with Democrats most worried about costs and Republicans about fraud. But that’s no guarantee of victory. Nirav Shah, an epidemiologist who led Maine’s top public health agency through the pandemic, lost a narrow Democratic primary in the state governor’s race in June.
Here are some of the public health officials on the ballot this year:
Xavier Becerra, Running for Governor in California

Becerra, who served as HHS secretary under President Joe Biden, is the highest-ranking former health official running this cycle. He won a crowded and expensive open primary and now faces Republican Steve Hilton, a British-born former Fox News host, in the general election.
Mark Peterson, a public policy professor at the UCLA Luskin School of Public Affairs, said with the pandemic in the rearview mirror, any judgment voters may have about the federal government’s response is more likely to reflect on Biden rather than Becerra, who has no medical background and maintained a low profile as HHS secretary.
Leading the nation’s health department as the pandemic lingered, Becerra focused more on expanding access to the Affordable Care Act and Medicaid, overseeing record numbers of people enrolled in the publicly financed programs during his tenure. He did face criticism over the processing and placement of a massive influx of migrant children at the U.S.-Mexico border, as well as his agency’s response to a baby formula shortage brought on, in part, by major product recalls.
Becerra has said he now wants to be California’s “healthcare governor,” a mantle outgoing Gov. Gavin Newsom tried to claim upon taking office in 2019.
Becerra’s campaign did not respond to a request for comment.
Before becoming HHS secretary, Becerra served as California’s attorney general and sued the first Trump administration more than 100 times, leading a coalition of states against GOP efforts to gut the ACA. He also started a unit in his office focused solely on healthcare. During Becerra’s tenure, his office reached a $575 million antitrust settlement with the California hospital system Sutter Health, pursued pharmaceutical companies that delayed generic drugs, and helped block a Trump administration rule that let employers choose whether to cover birth control.
Voters often regard decades of experience in government as a negative, Peterson said. But for the job of running the nation’s most populous state and the world’s fourth-largest economy, he added, “I think there are a lot of people out there who would like to have somebody who actually has run a big enterprise.”
In televised debates, Becerra has said California should maintain state-funded Medicaid coverage for immigrants without legal status. He is also a longtime supporter of implementing single-payer healthcare, though in recent interviews he has said it needs to be addressed at the federal level.
Amy Acton, Running for Governor in Ohio

Acton ran Ohio’s health department from February 2019 to June 2020.
During the first months of the pandemic, Acton appeared at daily news conferences with the state’s Republican governor, Mike DeWine, that were jokingly dubbed “Wine With DeWine.” She earned fans with her calm and positive demeanor while explaining her approach to keeping covid at bay.
But she also attracted critics with her recommendations to stay at home, mask up, and shut down some businesses to curb the virus’ spread. Protesters even showed up at her home.
Acton’s Republican opponent in the governor’s race, Vivek Ramaswamy, has labeled her “Dr. Lockdown” on social media. His criticism of her role in shutting down businesses could prove effective with the economy at the top of many people’s minds, said Christopher Devine, a University of Dayton political science professor.
“It’s a double-edged sword, because she also really upset some people,” Devine said of Acton’s time as the health director during the pandemic.
He said that is a tricky attack for Ramaswamy to pursue, though, because DeWine — still the sitting governor and a popular conservative figure — endorsed the covid measures Acton recommended, granting her emergency powers to sign the orders, and has since said he takes all responsibility for those actions.
For her part, Acton has done little on the campaign trail to highlight her time as the state’s public health director. Instead, she has focused more on healthcare affordability, highlighting the Trump-led cuts to Medicaid and the scaled-back subsidies for ACA plans that have resulted in thousands of people dropping coverage in the state.
“I hear from families across Ohio that healthcare costs are rising and they just can’t keep up,” Acton said in an emailed statement. “That’s why I will fight to protect and expand access, reduce the price of prescription drugs, forgive medical debt holding Ohioans back, and lower premiums.”
Abdul El-Sayed, Running for U.S. Senate in Michigan

El-Sayed — who ran the health departments in the city of Detroit and Wayne County, Michigan — is one of two leading Democratic candidates for Senate. The primary is Aug. 4.
El-Sayed, a progressive, is facing off against Haley Stevens, a four-term congresswoman. They are vying to run against Republican nominee Mike Rogers, a former congressman, for the Senate seat held by retiring Democrat Gary Peters.
From 2015 to 2017, El-Sayed ran the Detroit Health Department, which had been gutted and privatized as part of the city’s 2013 bankruptcy. In his role, he led efforts to test Detroit schools for lead in the wake of the Flint water crisis and provide free eyeglasses to children in public schools.
From 2022 until 2025, he ran the health department in Wayne County, the state’s most populous county, which includes Detroit. In that job, he initiated a program to retire medical debt for thousands of residents and make naloxone available in public areas to reverse the effects of opioid overdoses.
In an interview with KFF Health News, El-Sayed said his public health experience helped him become an effective communicator and challenge corporations and the role they play in healthcare.
“Politics have become overrun by big money and corporations, and my training and background in public health has taught me to think about that and push back against it,” he said.
El-Sayed, who did not practice medicine after completing his residency and is not licensed to do so, has faced criticism from some in his party for calling himself a doctor.
El-Sayed, who has endorsements from Sen. Bernie Sanders (I-Vt.) and U.S. Rep. Alexandria Ocasio-Cortez (D-N.Y.), supports “Medicare for All,” a policy favored by many progressives that would make more people eligible for the federal health program for people who are 65 and older or disabled.
David Dulio, a professor of political science at Oakland University in Rochester, Michigan, said that the broader economy, Trump’s tariffs, and trade are eclipsing healthcare this year as top concerns for voters in the state. But he added that “progressive stances such as Medicare for All are attractive in the Democratic primary electorate.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.This article first appeared on KFF Health News and is republished here under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
RoseRoseRoseOne of America’s most competitive gubernatorial races could settle a heated argument over whether private insurance companies should run Medicaid.
The race is in Iowa, whose Medicaid program has been plagued with controversy since 2016, when the state hired national insurance companies to manage billions of dollars’ worth of benefits.
That shift was made by then-Gov. Terry Branstad, a Republican. With his executive order, Iowa joined most other states in privatizing the management of Medicaid, which covers healthcare for more than 67 million Americans with low incomes or disabilities.
The arguments have resurfaced this year during the competition to replace Republican Gov. Kim Reynolds, who was Branstad’s protégé and continued contracting with private companies to manage Medicaid benefits. Zach Lahn, the Republican candidate to succeed the retiring governor, supports the practice. Rob Sand, the Democratic candidate, wants to end it.
“It’s been a disaster,” said Sand, Iowa’s state auditor. “The number of complaints has been catastrophic.”
Pros and Cons
Supporters of privatization say the insurers, known as managed-care organizations, make Medicaid more effective and efficient. Critics contend the companies pad their profits by denying payment for crucial health services and by shortchanging agencies and professionals who provide care.
Iowa is among 41 states, plus the District of Columbia, that contract with outside companies to run at least part of their Medicaid programs. Overall, private insurers manage the benefits of more than three-quarters of Medicaid patients. Connecticut is the only state that has fully reversed course after privatizing its Medicaid system.
Sand has criticized privatized Medicaid for years. As state auditor, he published reports alleging that the national insurers systematically deny or delay payment for services to which Medicaid participants are entitled.
He has vowed not to renew state contracts with the three insurers managing care for more than 600,000 Iowans on Medicaid, which is jointly financed by the state and federal governments. He would resume having state employees review and pay bills from clinics, hospitals, and other healthcare providers.
Lahn told KFF Health News that Sand’s pledge to resume state administration of Medicaid “is the exact wrong idea.”
Lahn is a former activist for Americans for Prosperity, a national pro-business group affiliated with the Koch family. He contends that state governments and Medicaid participants benefit when insurers compete to serve them.
“There are very few things that government does more efficiently than the private sector,” he said.
Lahn, who is a businessman and farmer, emphasized that state officials should strictly enforce contract requirements, ensuring that the insurers treat Medicaid recipients fairly and make prompt payments to care providers. He also said he would bar insurers from using artificial intelligence systems to determine whether to pay for medical claims under Medicaid. “Iowans deserve to have a human looking at their case,” he said.
Sand said in a recent interview that he doesn’t want Iowa to fully return to a “fee-for-service” Medicaid system, in which hospitals, clinics, and other healthcare agencies would effectively be paid piecemeal for whatever services they provided. Instead, he said, state employees should take over operation of a managed-care system, in which administrators review services to help ensure Medicaid participants receive what they need without wasting public money on ineffective services.
A few months ago, Republicans controlling the Iowa Legislature considered a bill to require the state to have a privately managed Medicaid system. That proposal would have blocked future governors from unilaterally shifting back to public management of the program. But the bill failed to pass.
Sand, a former assistant state attorney general, said he is confident he would have legal authority as governor to stop contracting with private Medicaid managers, although he cautioned that the transition would be complicated and could take time.


A Toss-Up Race
National political observers say the Iowa governor’s race could go either way.
This June, Lahn won an underdog primary campaign to beat a sitting congressman backed by President Donald Trump. Lahn gained Trump’s endorsement after winning the Republican primary. He is a vocal supporter of the Make America Healthy Again movement, led by Health and Human Services Secretary Robert F. Kennedy Jr., which aims to improve Americans’ diets and reduce environmental poisons.
Sand noted that Lahn’s past political activism included a failed 2014 attempt to defeat a proposal to cover more people under Montana’s Medicaid program.
Lahn said that at the time he worried the federal government would reduce how much money it would contribute to such Medicaid expansions, leaving states to foot much of the bill. He said he also didn’t want to see public programs such as Medicaid giving benefits to adults capable of providing for themselves. But he said those concerns have been allayed, partly by the Trump administration’s moves to require millions of Medicaid recipients to prove they are working, volunteering, or going to school.
If elected governor, he said, he would not try to reverse Iowa’s expansion of Medicaid, which happened in 2014 under Branstad.
Branstad also is the governor who decided in 2016 to hire private insurers to manage Medicaid.
Branstad, who declined to comment for this article, did not need the legislature to approve his momentous decision. He weathered controversy over the change, including allegations that the companies systematically denied payment for care that people with disabilities needed to remain in their homes.
Andy Schneider, a Georgetown University researcher who studies health policy issues, said it’s understandable that many government leaders see an advantage in hiring private Medicaid management companies. Each state’s Medicaid program pays claims for hundreds of thousands or even millions of members, and administrators must scrutinize bills from thousands of hospitals, clinics, and other healthcare organizations. “That’s a heavy lift,” said Schneider, who worked in federal Medicaid administration when Barack Obama was president.
Schneider noted that Medicaid expenses are among the biggest parts of any state’s budget. The costs can vary dramatically year to year, he said, which is hard for legislators and governors to plan for. Management companies sign contracts for set amounts of money per enrollee, depending on people’s ages and health conditions. Managed-care companies say they can improve Medicaid members’ health and reduce expenses. But Schneider said outside researchers have been unable to confirm or disprove those claims.
Federal law gives states flexibility in how they run their Medicaid programs, including whether they hire private insurers to manage the programs. “Unwinding those arrangements might take a little time, but there’s no question they can do it,” Schneider said.
Connecticut ended its use of private insurers to run Medicaid in 2012. Minnesota legislators decided to contract only with nonprofit insurers, starting in 2025, and that state’s governor has talked about doing away with private management altogether.
Gary Jessee, a former Texas Medicaid director who helped transition that state’s program into managed care, noted that most Americans’ health coverage is managed by some kind of insurance company, whether they obtain it on their own or get it through a government or employer plan.
Jessee now helps run a health policy consulting company whose clients include Medicaid managed-care companies. He said states rarely talk about totally scrapping contracts with such companies. Instead, he said, states have options to change the contracts, including to increase oversight or limit profits.
Overall, Jessee said, managed-care companies help Medicaid enrollees obtain the services they need to stay healthy. But it’s hard to calculate how much money the companies save states, he said, because all healthcare costs have been rising, and new members of managed-care plans may at first use more services as the insurance companies encourage them to get regular checkups instead of waiting for emergencies.
Iowa’s Medicaid program is managed by three insurers: Molina Healthcare, Elevance Health subsidiary Wellpoint, and Centene subsidiary Iowa Total Care.
None responded to requests for comment for this article.
Catherine Gray of Des Moines helps run a Facebook page for families who use Iowa’s Medicaid system. Her adult son, John, is on Medicaid because of a disability. Gray said the managed-care companies have made it much harder for people to obtain services, including mental healthcare, dental care, and transportation to health appointments. Iowa’s shift to the private system was abrupt and chaotic, she said. “We know people have died,” she said.
Gray said she probably will vote for Sand for governor, even though she doesn’t agree with every nuance of his stance on Medicaid. She suspects many other Iowans who use the program will do the same. “They’ve really been put through the wringer for 10 years, and they’re exhausted.”
This article first appeared on KFF Health News and is republished here under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.